No cure currently exists for COVID-19. People survive the virus because their own immune systems fight it off: thanks to, among other things, antibodies made by the body that bind to and neutralize virus particles. Now researchers at Columbia University have identified antibodies in hospitalized COVID-19 patients that could form the basis of medicines to help others.
Principal Investigator Larry Shapiro, PhD, at Columbia’s Zuckerman Institute, as co-senior author with David Ho, MD, published this work last month in Nature. Dr. Shapiro spoke with us about antibody cocktails, electron microscopes and hamsters.
How is this project aiming to combat COVID-19?
There has been a lot of talk about developing a vaccine. Vaccines can prevent infection by teaching the body to recognize and attack the virus. But so far, no vaccine has yet been approved to ward off COVID-19. In addition, even after a first-generation vaccine has been deployed, it’s likely that there will still be some infection and disease for some time.
So we’ve been exploring a different approach that might be faster to develop and deploy: antibody therapeutics. When someone is infected with a virus, their body tries to make antibodies to fight it off. There’s a sort of mini-evolution that takes place in our immune systems to produce each antibody. And some people make better antibodies than others.
We have been isolating antibodies from COVID-19 patients hospitalized at Columbia with Dr. Ho, scientific director of the Aaron Diamond AIDS Research Center and professor of medicine at Columbia University Vagelos College of Physicians and Surgeons. Our goal was to find antibodies that are particularly good at neutralizing the SARS-CoV-2 virus that causes COVID-19. We hope to develop preventative measures and treatments by administering those antibodies to people – as a prophylactic for high-risk individuals such as front-line healthcare responders who are healthy, and as a therapeutic for those who may have been exposed to the virus and for those who have become sick.
We hope to develop preventative measures and treatments by administering those antibodies to people.
How did you search for neutralizing antibodies?
We started by drawing blood from a large group of hospitalized patients. First, we tested the serum – the liquid component of blood that contains antibodies – from dozens of patients, and found that the responses of different people varied widely: only a small number had potently neutralizing serum. We continued our studies with blood samples from the five patients with the highest serum virus neutralization. We then turned to the cellular components of the blood. Antibodies are produced by cells called B cells; each B cell produces only one kind of antibody, so if you can isolate the B cell, you can get the antibody from that cell by RNA sequencing.
To isolate the right B cells – those that produce antibodies that recognize the virus – we used a piece of the virus: specifically, the viral spike protein. If you’ve ever seen an illustration of the coronavirus, you’ve seen this protein. It’s the one that sticks out all over the virus surface. The spike protein enables COVID-19 to bind to cells and then to fuse with the cell to release the virus’ genetic material and establish infection.
Knowing the sequences of the antibodies from the virus-targeting B cells enabled us to produce each antibody as a functional protein. We then ran experiments to see if the antibodies could not just bind to, but also neutralize the virus in a cell culture dish. This enabled us to identify a large set of potent virus-neutralizing antibodies.
Overall, serum from the blood of different individuals with COVID-19 varied over a wide range in its ability to neutralize the virus, revealing a wide range in the antibody response among those infected. People with the worst clinical effects, those infected for a long time and often having been on a ventilator, had stronger immune responses. Their antibodies appeared to be better at neutralizing the virus. This is something we’ve seen with HIV, a virus that I’ve spent many years studying.
What role did cryogenic electron microscope (cryoEM) technology play in this research?
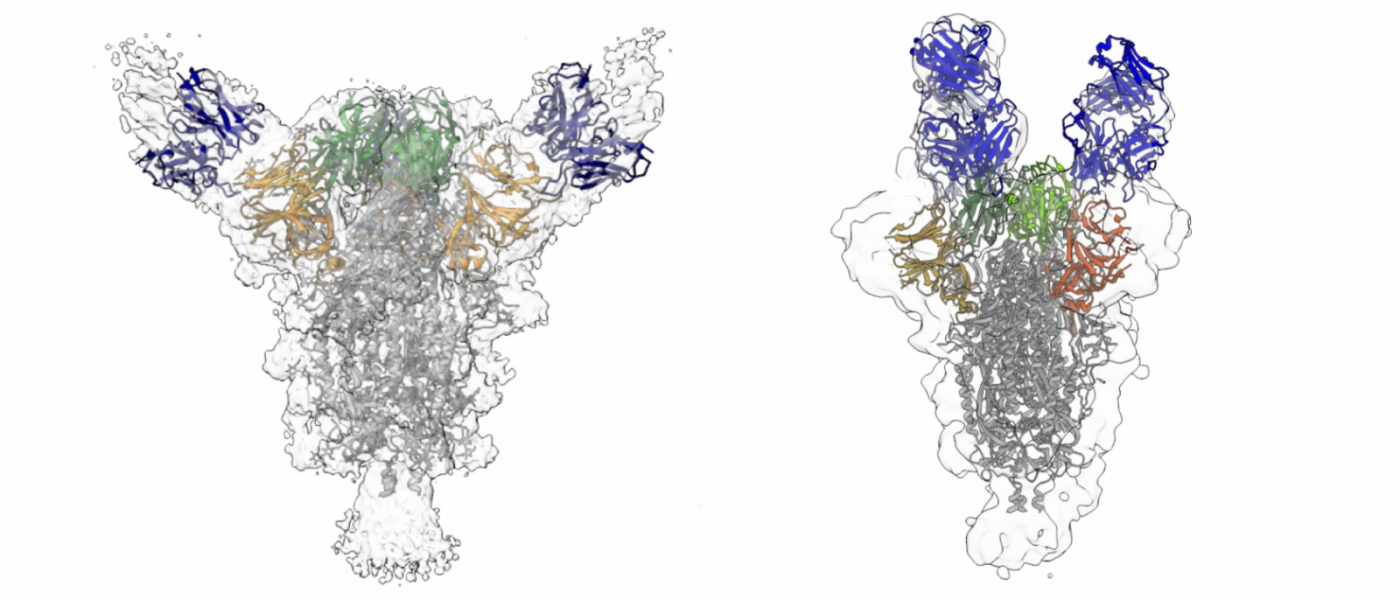
Cryo-EM, which uses a beam of electrons to probe samples, can show us the details of molecules at the atomic scale. With it, we were able to map where our antibodies bind on the spike. For one of the structures we published, we created an atomic-resolution model. We have a number of antibodies that bind to the spike very strongly but don’t neutralize the virus, and we’re looking at those too. Understanding why they don’t neutralize the virus has clinical implications. For example, if you know there’s one part of the virus that induces only non-neutralizing antibodies, you might want to get rid of that part in a vaccine.
Electron microscopy 3D reconstruction of antibody (blue) binding to viral spike protein (shaded gray, orange and green). (David Ho and Lawrence Shapiro | Columbia University)
Had others studied antibodies for SARS-CoV-2, the virus that causes COVID-19?
We’re not the first to isolate SARS-CoV-2 antibodies. Just in the month or so prior to our paper, other papers had reported on similar work. But we did something that wasn’t done for that previous research: We screened a large cohort of patients first, and we zeroed in on the ones who had the best neutralizing activity. So, I think that we were looking at a better set of donors.
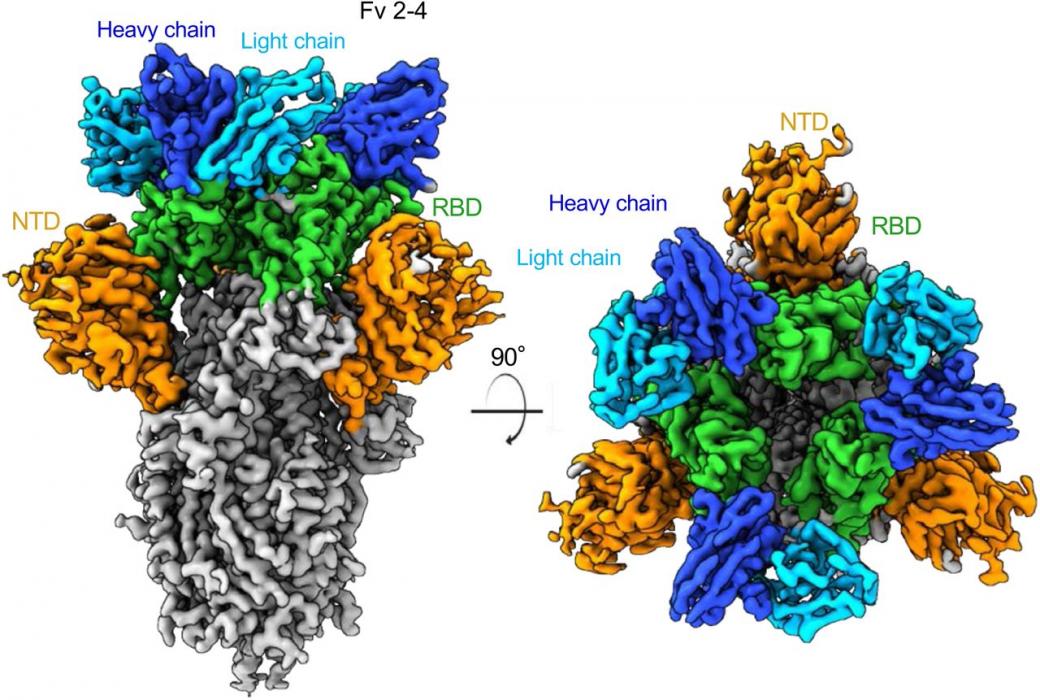
Also, there are a number of studies that used the receptor-binding domain, or RBD, of the spike protein to find their antibodies. We used the whole spike protein and found antibodies that target many different parts of the spike. So, in addition to antibodies that bind to the RBD, antibodies that bind to another part called the N-terminal domain, and antibodies that recognize both parts at once.
Could that lead to antibody cocktails: treatments that mix several different antibodies?
Exactly. One problem with viruses is that they tend to mutate. When a virus mutates, leading to a change in part of its structure, an antibody that used to bind to that part may no longer be able to do so. The more antibodies you have targeting different parts, the harder it is for the virus to avoid neutralization by mutating. That’s where antibody cocktails come in.
Others are attempting to make cocktails by using antibodies that target different regions of RBD. But RBD is a very small thing. We have antibodies for different regions across the spike, so that a mutation at one binding site won’t affect neutralization at another site. And so the virus has a very hard time escaping the antibodies. We’re looking at two or three antibody cocktails, each with two or three antibodies.
We’ve already seen very good results using only one antibody. At a very low dose, we were able to impart immunity to hamsters by injecting antibodies before exposing them to SARS-CoV-2. There was almost no virus detectable in their lungs, as we describe in our paper. It’s not clear what the efficacy will be for patients who are already in the worst stages of the disease. But I think that we’re much more confident about the preventative capabilities of neutralizing antibodies – their prophylactic capacity. And I think that ultimately we’ll probably look in clinical trials for both prophylactic and therapeutic use.
Once antibodies are discovered, how do they become medicine?
A pharmaceutical company will insert the antibody genes into a highly specialized mammalian cell line optimized to produce antibodies. These are grown in huge bioreactors, as kilograms of protein are required.
What were the hardest parts of this research?
I’m a structural biologist, so I’m worried about structures. When we first started looking at the CoV-2 spike protein, it was mostly unfolded. It was very difficult to work with because it flops around. Let me tell you how we got over that problem. We found that at the pH of blood, 7.4, the protein is somewhat unstable. But once it’s inside a part of the cell called an endosome, which has pH as low as 4.5, it becomes hard like a rock. So we used low-pH conditions to visualize the spike with cryo-EM. It’s much easier to visualize the rock-like spike protein at pH 4.5 than the more wet-noodle-like spike at pH 7.4. Once we identified this solution, we were off to the races.
What are the next steps?
We’re looking at how this spike-shape-changing phenomenon helps the virus evade some potentially neutralizing antibodies. We’ve just submitted a paper that shows that when the spike protein changes shape in the low pH of the endosome, some spike-binding antibodies are knocked off. That gives the virus a way to fool the immune system into developing antibodies that won’t actually work. This finding could inform future vaccine designs. We’re also looking in greater detail at the antibody response in different people and trying to understand why it differs so much between individuals.
How does this work relate to your AIDS research?
Almost everything being done with COVID-19 was developed first for HIV. Vaccine development, cell-sorting, everything cut its teeth on HIV. If you look at the people who are making the contributions, a lot of them are people who grew up studying HIV and were able to transfer their expertise. It’s great to be able to contribute something that might have an actual clinical impact. That’s why I got into this in the first place.
###
The paper is titled “Potent neutralizing antibodies directed to multiple epitopes on SARS-CoV-2 spike.” Additional contributors include Lihong Liu, Pengfei Wang, Manoj S. Nair, Jian Yu, Micah Rapp, Qian Wang, Yang Luo, Jasper F-W. Chan, Vincent Sahi, Amir Figueroa, Xinzheng V. Guo, Gabriele Cerutti, Jude Bimela, Jason Gorman, Tongqing Zhou, Zhiwei Chen, Kwok-Yung Yuen, Peter D. Kwong, Joseph G. Sodroski, Michael T. Yin, Zizhang Sheng, and Yaoxing Huang.